Direct Primary Care (DPC):
Potential Impact on Cost, Quality, Health Outcomes,
and Provider Workforce Capacity
A Review of Existing Experience & Questions for Evaluation
Health Policy Programs Group
UW Health Policy Group 1 | 20
Table of Contents
I. Federal Law and DPCs.............................................................................................................. 2
II. State DPC Laws ........................................................................................................................ 3
III. Evaluations and Case Studies .................................................................................................. 7
IV. The Value Proposition for Purchasers and Consumers ........................................................... 8
A. Preventive Services Covered by Health Plans ........................................................................... 8
B. Value-Added Calculation for Consumers ................................................................................. 11
V. Health System Value: Utilization, Quality, Outcomes .......................................................... 14
A. Volume of Care and Utilization .................................................................................................. 14
B. Quality and Outcomes ................................................................................................................ 11
VI. How do DPCs Affect the Primary Care Workforce? ............................................................. 16
VII. Conclusion: Questions for Consideration ............................................................................ 19
VIII. Other Background Reading .................................................................................................. 20
UW Health Policy Group 2 | 20
Direct Primary Care (DPC) contracts, or “medical retainer agreements,” are a healthcare delivery model
where a provider offers unlimited specified routine health care services for a monthly fee.
1,2
Proponents
of DPC suggest that the delivery method will improve access to care, reduce administrative costs, foster
stronger patient-provider relationships, and reduce reliance on expensive emergency department
services. Critics of DPC contend that it double-charges for services already covered by insurance, and
that DPC contracts lack accountability for quality and access. This paper 1) describes proposed and
existing DPC bills, 2) reviews existing DPC experience and evaluations, and 3) considers what effect DPC
could have on health care in Wisconsin.
I. Federal Law and DPCs
Federal law concerning DPC arrangements falls into two main categories: DPC and the private insurance
market, and DPC and the Medicaid program.
DPC and the Private Insurance Market
The Patient Protection and Affordable Care Act (ACA) allows a qualified health plan (QHP) issuer to
“provide coverage through a direct primary care medical home…so long as the QHP meets all
requirements that are otherwise applicable and the services covered by the direct primary care medical
home are coordinated with the QHP issuer.” That is, DPC may be included in plans sold on the ACA
insurance exchanges, but must be paired with a wraparound insurance policy covering everything
outside of primary care.
3
In April 2018, the federal Centers for Medicare and Medicaid Services (CMS) released a public request
for information regarding DPC models for primary care and other specialties, titled “Direct Provider
Contracting.” That document is available here:
https://innovation.cms.gov/ini…/direct-provider-
contracting/. CMS solicited input on direct provider contracting between payers and primary care or
multi-specialty groups. This would inform potential testing of a DPC model within the Medicare fee-for-
service program (Medicare Parts A and B), Medicare Advantage program (Medicare Part C), and
Medicaid.
Current Internal Revenue Service (IRS) rules prohibit individuals with health savings accounts (HSAs)
paired with high deductible health plans (HDHPs) from having an agreement with a DPC provider. The
IRS interprets DPC arrangements as health plans under Section 223(c) of the Internal Revenue Code, The
law is unclear whether primary care services are qualified health expenses under Section 213(d) of the
1
Wisconsin Legislative Council, Amendment Memo, 2017 Senate Bill 670, Senate Substitute Amendment 1.
February 2, 2018. https://docs.legis.wisconsin.gov/2017/related/lcamendmemo/sb670.pdf
2
Chappell GE. 2017. Health Care’s Other “Big Deal”: Direct Primary Care Regulation In Contemporary American
Health Law. Duke Law Journal. Vol. 66: 1330-1370.
https://pdfs.semanticscholar.org/4774/9abed07d68ebbb7006599b15c568e62350c2.pdf
3
45 C.F.R. § 156.245; Dave Chase, Direct Primary Care: Regulatory Trends, FORBES (July 10, 2013),
http://www.forbes.com/sites/davechase/2013/07/10/direct-primary-care-regulatory-trends/
UW Health Policy Group 3 | 20
code if paid for as a capitated periodic fee rather than on a fee for service basis. IRS regulations require
HSAs be paired with an HDHP, and the HSA holder may not have a second health plan. The IRS
interpretation of DPC as a health plan bars an individual who has an agreement with a DPC provider
from funding an HSA.
A bipartisan bill in Congress, the Primary Care Enhancement Act (HR 365/S. 1358), clarifies the tax code
regarding the use of HSAs for DPC. The bill would clarify the tax code to allow patients with HSAs paired
with HDHPs to use those funds to pay for periodic fee-based DPC. As of June 2018, the House
Committee on Ways and Means has not yet considered this bill.
DPC and Medicaid
Federal Medicaid law specifies that that “The State Medicaid agency must require all ordering or
referring physicians or other professionals providing services under the State plan or under a waiver of
the plan in the fee-for-service program to be enrolled as participating Medicaid providers.”
4
A DPC
provider would need to be a Medicaid participating provider to serve Medicaid members. However,
CMS has determined that, in Medicaid risk-based managed care arrangements, states hold discretion
over provider enrollment requirements for the ordering or referring physicians.
5
An advocacy website
of a group that supports expansion of DPC contracts reviews questions that DPC practices have about
this CMS guidance.
6
II. State DPC Laws
Twenty-five states have passed legislation generally defining DPC outside of state insurance regulation.
7
This state action defines DPC as a medical service, not a health plan. Wisconsin, Georgia, Maryland,
Pennsylvania and South Carolina have introduced DPC legislation, but have not enacted those bills into
law. Montana Governor Steve Bullock is the only governor to have vetoed a DPC bill, doing so in 2017.
Discussion of the origin, history, and legislative framework for each state’s DPC bill are available from
other sources, with detailed tables as of 2017.
8,9
About half of enacted laws use the phrase “direct
primary care” while the other half use the substantively equivalent phrase “medical retainer
agreement.” All bills include language expressly stating that DPC is not insurance, and that DPC is not
4
42 CFR § 455.410(b)
5
CMS, DHHS. Cindy Mann, Director. Medicaid/CHIP Provider Screening and Enrollment. December 23, 2011.
https://www.medicaid.gov/Federal-Policy-Guidance/downloads/CIB-12-23-11.pdf
6
DPC Frontier. Medicaid – A Full Analysis. https://www.dpcfrontier.com/medicaid/
7
Details on these bills are available at https://www.dpcare.org/state-level-progress-and-issues.
8
Eskew P. Direct Primary Care Business of Insurance and State Law Considerations. Unpublished Paper.
https://static1.squarespace.com/static/54c15fbce4b06765d7d750d5/t/59cc42388fd4d26e72d28126/1506
558521439/Direct+Primary+Care+Business+of+Insurance+and+State+Law+ConsiderationsNYSBA.pdf
9
Appendix to Health Care’s Other “Big Deal”: Direct Primary Care Regulation in Contemporary American Health
Law Glenn E. Chappell 66 DUKE L.J. (March 2017)
https://pdfs.semanticscholar.org/4774/9abed07d68ebbb7006599b15c568e62350c2.pdf
UW Health Policy Group 4 | 20
subject to regulation by the state’s Insurance Commissioner or other state insurance regulators. Each of
these laws defines DPC similarly, as an agreement between a primary care provider and a patient to
provide unlimited access to primary care services in exchange for an agreed-upon monthly fee for an
agreed-upon period. Various state laws address other elements. Alabama, for example, expressly
includes dentists as providers covered under the bill. The Direct Primary Care Coalition, a group that
advocates for expansion of DPC, has drafted model DPC legislation.
10
In theory, DPC paired with a wrap-around health plan, may be offered in ACA exchanges, by self-insured
employers, unions, and by Medicare Advantage and Medicaid managed care organizations. State laws
vary in whether they allow DPCs to engage in third-party billing, or the ability of DPC providers to
receive reimbursement from private insurers or state Medicaid agencies:
• Only Washington and Louisiana allow insurer reimbursement for member DPC subscriptions.
• Michigan,
11
Nebraska,
12
Louisiana,
13
and West Virginia
14
have statutory language that permit
Medicaid payments for DPCs, while Mississippi and Texas preclude DPCs from billing Medicaid.
15
• Missouri, Arkansas, and Oklahoma do not prohibit DPCs from billing insurers for services.
Missouri’s law expressly allows payments from health savings accounts, flexible spending
arrangements, or health reimbursement arrangements.
State Pilot Programs
In 2006, West Virginia enacted the Preventive and Primary Care Pilot Program to provide such services
to the uninsured for a prepaid fee (West Virginia Code § 16-2J.)
16
The law specified that health care
providers in this program were not providing insurance or offering insurance services. A DPC advocate
reviewed the West Virginia program and how various elements, such as limiting its scope to the
uninsured population, might restrict the success of DPC practices.
17
That writer compared the West
Virginia provisions to a DPC law passed in 2007 by State of Washington, and concluded that
Washington’s legislation, along with elements of other states’ laws, better promotes successful DPC
practice:
States considering passing similar legislation should consider enacting a hybrid of the West
Virginia, Washington, Utah, and Oregon statutes, taking the most helpful portions from each.
Physicians should be able to market their services directly to patients or employers without
regard to the current insurance status. Avoiding unneeded scope of service restrictions will
10
https://www.dpcare.org/dpcc-model-legislation
11
Michigan Public Act 158 of 2017
12
Nebraska Neb. Rev.St. § 71-9510.
13
La. Stat. § 37:1360.85.
14
W. Va. Code. § 30-3F-2.
15
Miss. Code Ann. § 83-81-3(c) (2015); Tex. Occ. Code § 162.254 (2015).
16
West Virginia Health Care Authority. Primary Care Pilot Program.
https://hca.wv.gov/primarycare/Pages/default.aspx
17
Eskew P. Direct Primary Care Membership Medicine. West Virginia Medical Journal. March/April 2014 Vol. 110:
8-11. http://cdn.coverstand.com/30875/197958/83364ec4719c32123930be5019940709e1e49d59.5.pdf
UW Health Policy Group 5 | 20
magnify the economic benefits experienced by patients of the DPCMM practices. Rules regarding
the acceptance of new patients and discontinuing care are helpful, and the Washington
legislation provides an excellent example in this regard.
West Virginia renewed its pilot program through 2016, then adopted a new statutory provision for
Direct Primary Care Practice in 2017. The new law allows that, while a provider may not bill third parties
for services rendered under the DPC agreement, “[a] primary care provider may accept payment for
medical services or medical products provided to a Medicaid or Medicare beneficiary” and
“[a] patient or legal representative does not forfeit insurance benefits, Medicaid benefits or Medicare
benefits by purchasing medical services or medical products outside the system.”
18
Michigan’s legislature, in 2017, directed its Medicaid agency to apply to CMS for a waiver to allow DPC
for Medicaid enrollees.
19
The legislature appropriated funds for a one-year DPC pilot program, to
include no more than 400 enrollees across various Medicaid eligibility categories. Michigan has not yet
implemented the pilot program, and the Michigan Medicaid agency reports that the timeframe depends
on negotiations between the Medicaid health plans and any potential contracted providers.
The State of Nebraska codified DPC in state law, with the Governor signing 2015 NE L.B. 817 into law in
March 2016. With DPC available on the commercial market, Nebraska’s legislature introduced NE L.B.
1119,
20
which the Governor signed in April 2018 as the Direct Primary Care Pilot Program Act. The
program begins in fiscal year 2019-2020 and runs through fiscal year 2021-2022. This law requires the
State Health Insurance Program to include two direct primary care coverage options for participating
state employees.
21
Wisconsin DPC Bills: 2017 AB 798 and SB 670
Wisconsin’s 2017 Assembly Bill 798 (AB 798) was introduced in December 2017, along with companion
Senate Bill 670 (SB 670).
22
The Senate Committee on Public Benefits, and the Assembly Committee on
Small Business Development passed identical substitute amendments to SB 670 and AB 798,
respectively, in February 2018.
23
The full Assembly passed AB 798, as amended, but the Senate did not
take up the bill before the end of the legislative session, and the proposal was not enacted into law.
18
W. Va. Code § 30-3F-2. See also: West Virginia Board of Medicine, Direct Primary Care Practice.
https://wvbom.wv.gov/Direct_Primary_Care_Practice.asp#30-3F-2
19
Michigan Department of Health and Human Services. Implementation of the Direct Primary Care Pilot Program,
Quarterly Report 1. January 19, 2018.
https://www.michigan.gov/documents/mdhhs/Section_14078_PA_158_of_2017_Quarterly_Rpt_1_6148
60_7.pdf
20
https://nebraskalegislature.gov/bills/view_bill.php?DocumentID=34744
21
Office of Governor Pete Ricketts, State of Nebraska. Gov. Ricketts Signs Legislation Expanding Healthcare
Options. April 13, 2018.
https://governor.nebraska.gov/press/gov-ricketts-signs-legislation-expanding-
healthcare-options
22
https://docs.legis.wisconsin.gov/2017/proposals/sb670
23
https://docs.legis.wisconsin.gov/2017/related/amendments/sb670/ssa1_sb670

UW Health Policy Group 6 | 20
The original bill would have specified that DPC does not fall under regulation as an insurance plan, and
required that the Wisconsin Department of Health Services (DHS) establish and implement a DPC
program for Medicaid enrollees. The Legislative Reference Bureau summarizes SB 670 as follows:
The bill allows a health care provider and an individual patient or employer to enter into a direct
primary care agreement and requires the Department of Health Services to establish and
implement a direct primary care program for Medical Assistance recipients. A direct primary care
agreement is a contract in which the health care provider agrees to provide routine health
services such as screening, assessment, diagnosis, and treatment for the purpose of promotion of
health or the detection and management of disease or injury, dispensing of medical supplies and
prescription drugs, and certain laboratory services for a specified fee over a specified duration. A
valid direct primary care agreement outside of the Medical Assistance program must, among
other things, state that the agreement is not health insurance and that the agreement alone
may not satisfy individual or employer insurance coverage requirements under federal law. The
bill exempts direct primary care agreements from the application of insurance law. The bill also
allows DHS to investigate complaints related to private direct primary care agreements.
Services. The bill defines “routine health care service” to mean screening, assessment, diagnosis,
and treatment for the purpose of promotion of health or the detection and treatment for the
purpose of promotion of health or the detection and management of disease or injury. The substitute
amendment removed the bill’s specific provisions on laboratory services and dispensing of medical
supplies and prescription drugs.
Medicaid Pilot Program
The Wisconsin Legislative Council summarizes the provisions of the bill and substitute amendment as
follows:
The bill requires the Department of Health Services (DHS) to contract with one or more primary
care providers to implement a direct primary care program for MA recipients. DHS must
enter participants into a direct primary care agreement to receive routine health services from
one of these providers for a monthly fee, as will be specified in the agreement. After the program
is implemented, DHS must submit annual reports to the Legislature.
The substitute amendment removes these provisions and instead requires DHS to convene a
work group to propose a direct primary care pilot program. A hearing must be held on the
proposal, and legislation must be introduced following the hearing. The work group is also
directed to submit a report regarding implementation of an “alternative payment model” for
potentially preventable hospital readmissions of MA recipients.
The bill text, prior to removal by substitute amendment, contemplates how the Medicaid pilot might
operate, specifically noting an average fee of $70 per month.
UW Health Policy Group 7 | 20
III. Evaluations and Case Studies
This existing scholarly literature on DPCs provides descriptive and survey information,
24
but generally
lacks rigorous studies on cost, quality, and outcomes.
25
One study assessed the effect of the personalized health care model used by MD-Value in Prevention
(MDVIP), a collective direct primary care group with practices in 43 states and the District of
Columbia).
26
This study reported substantial savings per patient, mostly because of reductions in
hospital utilization. But the study did not adjust for baseline health or socioeconomic factors of its
members relative to comparison population – factors that would affect health care use. This study,
therefore, does not allow conclusion about the impact of the delivery model.
The Qliance Medical Group has received perhaps the most attention in the literature. Founded in 2007
in Seattle, Qliance established itself as the nation’s largest DPC healthcare consortia. Supported by
Washington State’s permissive DPC law, Qliance served individuals, employers, and Medicaid
members.
27
In 2014, the company became the nation’s first DPC provider to join the ACA health
insurance exchange. By 2015, Qliance groups served 35,000 patients in the Seattle area, half of whom
Medicaid covered.
28
Qliance had early success with market expansion, but faltered financially and, by 2017, had closed all
clinic operations.
29
The Qliance Medical Group filed for Chapter 7 bankruptcy on May 7, 2018.
30
The
payment levels apparently proved insufficient to cover the DPC costs. Others have voiced this concern:
One 2015 review of existing DPC practices reported that DPCs charged patients an average $77.38 per
month,
31
while another reported monthly rates between $42 and $125.
32
Such rates fall substantially
24
https://www.dpcfrontier.com/academic-articles
25
Cole E. Direct Primary Care: Applying Theory to Potential Changes in Delivery and Outcomes. J Am Board Fam
Med July-August 2018; 31:605-611
26
Klemes A, Seligmann RE, Allen L, Kubica MA. Warth K Kaminetsky B Personalized preventive care leads to
significant reductions in hospital utilization. Am J Manag Care., 2012, vol. 18:e453-60.
27
Qliance and Healthcare Reform Fact Sheet for Individuals
http://qliance.com/wp-content/uploads/2011/10/Qliance-and-Healthcare-Reform-Fact-Sheet_Final.pdf
28
von Drehle D. Medicine Is About to Get Personal, TIME, Dec. 22, 2014. http://time.com/3643841/medicine-
gets-personal
29
Andrews M. A Pioneer In 'Flat-Fee Primary Care' Had To Close Its Clinics. What Went Wrong? NPR Shots. June 20,
2017.
https://www.npr.org/sections/health-shots/2017/06/20/533562142/a-pioneer-in-flat-fee-primary-
care-had-to-close-its-clinics-what-went-wrong
30
Ellison A. Direct primary care group files for bankruptcy after abruptly closing clinics. Becker’s Hospital Review.
May 30, 2018.
https://www.beckershospitalreview.com/finance/direct-primary-care-group-files-for-
bankruptcy-after-abruptly-closing-clinics.html
31
Eskew P, Klink K. Direct Primary Care: Practice Distribution and Cost Across the Nation. JABFM, Journal of the
American Board of Family Medicine. November–December 2015 Vol. 28 No. 6.
http://www.jabfm.org/content/28/6/793
32
Rowe K, Rowe W, Umbehr J, Dong F, Ablah E. Direct Primary Care in 2015: A Survey with Selected Comparisons
to 2005 Survey Data. Kansas Journal of Medicine. 2017;10(1):3-6.
UW Health Policy Group 8 | 20
short of the average of $182.76 per month charged by "concierge" or "boutique" medical practices,
which also usually bill insurers for their services.
The literature includes descriptive reports of Qliance early operations,
33
but offers no independent
evaluations of Qliance performance. Qliance, in a 2015 press release, announced that its model “delivers
20% lower overall healthcare costs, increases patient satisfaction, and delivers better care.”
34
Qliance
attributed these savings to a substantial reduction in ER visits, inpatient days, specialist visits, advanced
radiology visits, along with more primary care visits.
However, external evaluators did not conduct the Qliance study. The study was not subject to peer
review, and was not published in a scientific journal. It does not specify whether the underlying risk
status differed between those who joined Qliance relative to a comparison group, how long the Qliance
members had been with Qliance, or whether the Qliance members might have visited any providers
outside of their Qliance contract that went unrecorded in the study. For these reasons, the Qliance’s
reported results may not be attributable to the DPC as a delivery model. DPC may attract a lower risk
member population, and some observers suggest that unlimited primary care encourages the "worried
well" to get more care than they need, but does not necessarily promote evidence-based services that
improve health.
IV. The Value Proposition for Purchasers and Consumers
DPC offers a potential value proposition in two regards: potential savings in health care costs, and
improved patient experience and satisfaction. DPC proponents point to potential benefits for the health
care system, through a reduction in overall health insurance premiums or health care payments if the
DPC can avert unnecessary referral, specialty, hospital, imaging, laboratory, prescription drug costs and
other services. DPC’s value proposition to consumer: expansive access to a primary care provider and all
services provided within that provider’s practice, and longer visit times with their health care provider,
potentially improving the health care experience.
Ultimately, the value to both purchaser and consumer depends on whether the model reduces financial
outlays and improves health outcomes. This section looks at the DPC interaction with other insurance
benefits and the potential to deliver cost savings to the consumer.
A. Preventive Services Covered by Health Plans
A low-risk consumer could likely get many, if not most, needs met through their primary care provider.
That consumer would then need to get a wrap-around plan with a high deductible and co-payments in
the event of a hospitalization or need for specialist services. However, with the ACA’s preventive
services requirement, that plan will already provide coverage for most of the screening and preventive
33
Wu WN, Bliss G, Bliss EB, Green LA. Practice profile. A direct primary care medical home: the Qliance experience.
Health Aff (Millwood). 2010;29(5):959–962.
34
Qliance. New Primary Care Model Delivers 20 Percent Lower Overall Healthcare Costs, Increases Patient
Satisfaction and Delivers Better Care. January 15, 2015.
https://www.prnewswire.com/news-
releases/new-primary-care-model-delivers-20-percent-lower-overall-healthcare-costs-increases-patient-
satisfaction-and-delivers-better-care-300021116.html

UW Health Policy Group 9 | 20
services that the DPC would also provide. The question here becomes whether the DPC subscription fee
adds value beyond the preventive services already built into any other coverage that includes mandated
preventive services.
The ACA requires that private insurance plans cover recommended preventive services without any
patient cost-sharing.
35
This means that consumers paying for both insurance and DPC will be paying
twice for those services, unless the insurance plan can carve out the required preventive service benefit
and use the DPC provider to fulfill the requirement.
In 2013, the IRS confirmed that high-deductible health plans (HDHPs) also must cover all preventive
services mandated under the ACA without imposing a deductible.
36
Private health plans must cover a
range of preventive services and may not impose cost-sharing (such as copayments, deductibles, or co-
insurance) on patients receiving these services. These requirements apply to all private plans – including
individual, small group, large group, and self-insured, except plans that maintain “grandfathered” status.
To have been classified as “grandfathered,” plans must have existed prior to March 23, 2010, and
cannot make significant changes to their coverage (for example, increasing patient cost-sharing, cutting
benefits, or reducing employer contributions).
The clinical preventive services fall into four categories
37
: 1) Evidence-Based Screenings and Counseling,
2) Routine immunizations, 3) Preventive Services for Children and Youth, and 4) Preventive Services for
Women.
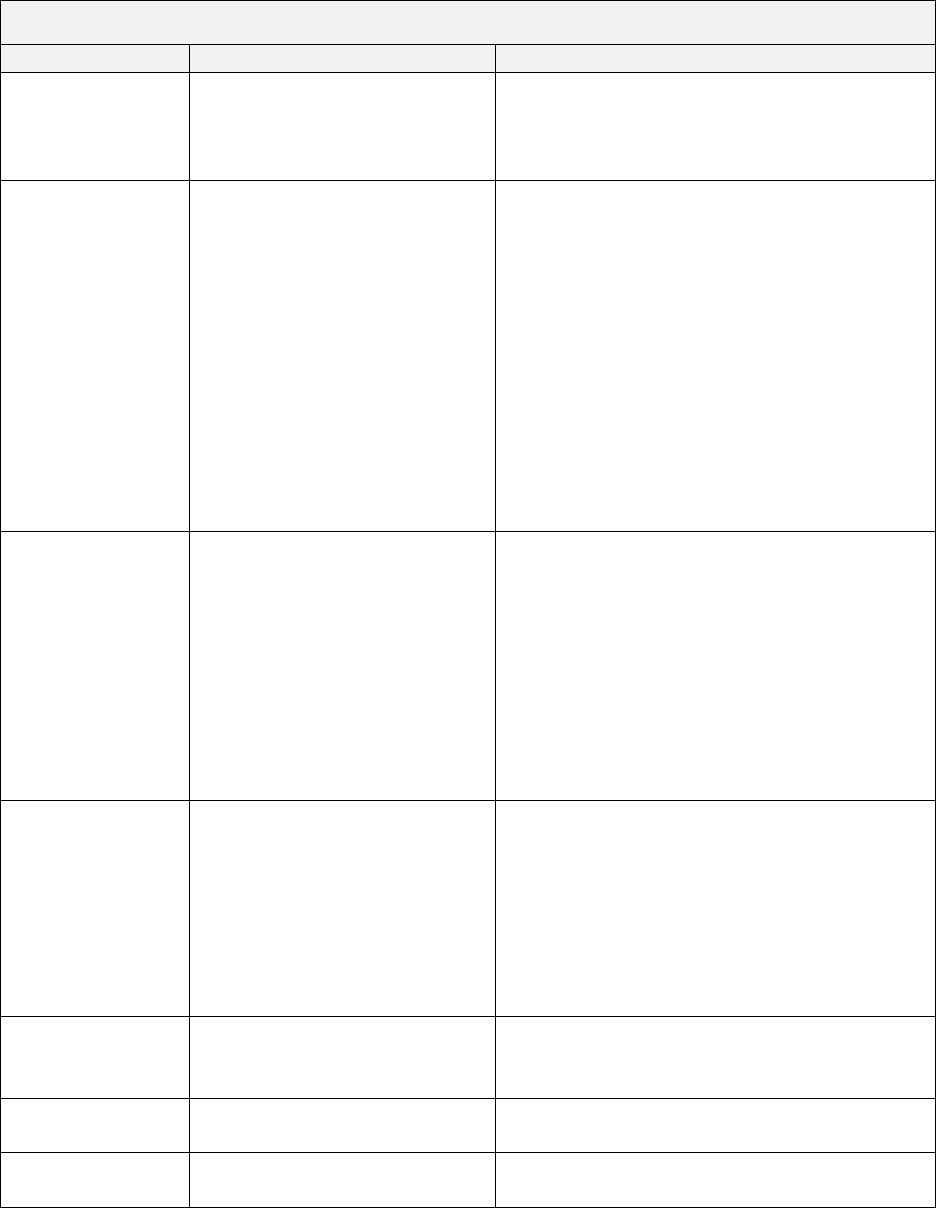
Table 1 compares the coverage that consumers might have for services under a DPC agreement, as
defined by SB 670, relative to what they would have under standard health plan. A consumer within a
DPC agreement would presumably also purchase a complimentary “wrap-around” health plan to cover
the services not provided within by the DPC contract, including most prescription drugs, laboratory,
specialist, and hospitalization services. The degree to which a consumer would use such coverage would
will depend on risk profile and the consumer’s pre-existing health conditions.
35
Healthcare.gov. Preventive health services. https://www.healthcare.gov/coverage/preventive-care-benefits/
See also: Preventive Services Covered under the Affordable Care Act. Quartz.
https://unityhealth.com/docs/default-source/docs/acapreventiveservices.pdf?sfvrsn=2
36
IRS Notice 2013-57. https://www.irs.gov/pub/irs-drop/n-13-57.pdf
37
For detail, see https://www.kff.org/health-reform/fact-sheet/preventive-services-covered-by-private-health-
plans/#endnote_link_160040-3
UW Health Policy Group 10 | 20
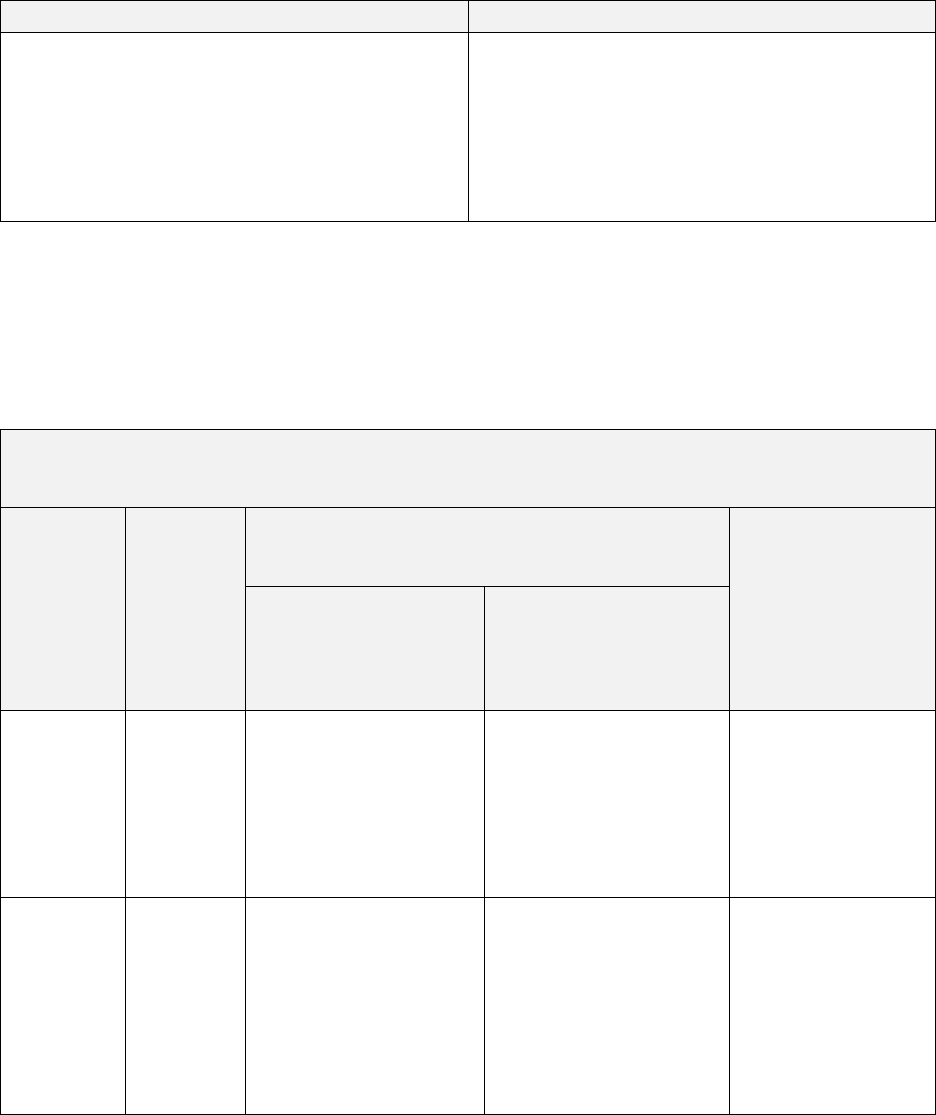
Table 1. Services Covered under DPC Contract and under Standard Health Plan Coverage
Services
Direct Primary Care
Standard Health Plan Coverage
Screening
No additional cost to consumer
for screening services that fall
within the scope of the DPC’s
ability and scope.
No out-of-pocket cost to the consumer; most
screening services will fall within the ACA’s
preventive services mandate and therefore
would be covered.
Assessment,
Diagnosis, and
Treatment
No additional cost to consumer
for assessment, diagnosis, and
treatment services that fall
within the scope of the DPC’s
ability and scope.
Consumer remains exposed to
full cost for assessment,
diagnosis, and treatment
services by other providers
beyond the DPC, including
referrals, specialists, and
second opinions.
No out-of-pocket cost to consumer for some
assessment, diagnosis, and treatment that
occur incidental to the preventive services.
For example, removal of polyps during a
routine colonoscopy would be included as a
“free preventive service.”
Other office visits, assessment, diagnosis, and
treatment services would be covered, often
pre-deductive and subject to a co-payment.
Dispensing of
Medical Supplies
and Prescription
Drugs
Limited only to product
dispensed directly within the
clinic by the DPC provider.
Consumer remains fully
exposed to most prescription
drug costs, as those are
generally dispensed by a
licensed pharmacy outside of
the primary care office setting.
Covered, subject to health plan’s cost-sharing
and deductible provisions. Many prescription
drugs covered prior pre-deductible, subject to
co-payment.
Laboratory
services, including
routine blood
screening and
routine pathology
screening
No coverage for any laboratory
services that fall outside of the
DPC’s on-site lab or the lab that
has entered into an agreement
with the DPC.
Some laboratory services that fall within the
ACA ‘s preventive services mandates covered
at no out-of-pocket cost to consumer:
Other laboratory services covered, some pre-
deductible, subject to health plan copayment
and deductible provisions.
Specialist services
No coverage
Covered, some pre-deductible, subject to
health plan co-payment and deductible
provisions
Emergency
Department
No coverage
Covered, subject to health plan co-payment
and deductible provisions
Hospitalization
No coverage
Covered, subject to health plan co-payment
and deductible provisions
UW Health Policy Group 11 | 20
B. Value-Added Calculation for Consumers
The monetary value of a DPC arrangement to a consumer would depend on comparison of these two
cost bundles:
Situation 1: DPC plus HDHP/HSA
Situation 2: Standard Insurance Coverage
Costs to Consumer
• Monthly DPC fee
• Monthly HDHP premium with HSA deposits
• Out-of-Pocket costs for specialist, lab,
prescription drug, and hospitalization services
pre-deductible
Costs to Consumer
• Monthly premium for standard insurance
• Out-of-pocket costs not covered by standard
insurance.
Note also that the bills considered by the Legislature in the 2017-19 session specify that direct primary
care payments may not count towards the patient’s insurance deductibles or out-of-pocket expenses. A
consumer using an insurance plan rather than a DPC would have their payments for primary care
services applied toward any deductibles. Table 2 compares cost-exposure for a consumer across the
range of services, pre- and post- deductible.
Table 2: Sources of Coverage for Health Care Services,
DPC with HDHP compared to Standard Health Insurance Plan
Preventive
Services
(ACA
mandated)
Pre-Deductible
Post Deductible
Primary care
office visits:
Specialist, lab, imaging,
prescription, emergency
department
Situation 1:
DPC plus
HDHP
DPC fee
HDHP
covered
services
DPC subscription fee
Consumer out-of-pocket
(or HSA payments)
DPC fee
Cost-sharing
provisions for other
services, up to HPDP
out-of-pocket
maximum
Situation 2:
Standard
Insurance
Coverage
Standard
plan
covered
services
Covered pre-deductible,
often subject to co-
payments; copayments
applied toward
deductible
Pre-deductible, often
subject to co-pays;
emergency department
may or may not be
subject to deductible
copayments applied
toward deductible
Cost-sharing
provisions, up to
out-of-pocket
maximum
UW Health Policy Group 12 | 20
Private Market: Standard Insurance Coverage vs DPC-plus-HDHP
This section compares costs to the consumer for Situation 1 (DPC and HDHP insurance plan) and
Situation 2 (Standard non-HDHP plan).
A consumer in a DPC arrangement would have to pay the DPC fees, and decide whether to enroll in a
plan that offers coverage for services not included in the DPC contract, such as specialist and hospital
services. The relative monetary value will depend on whether a consumer has overall out-of-pocket
costs lower than what would be required under standard insurance after copayments, and restrictions
on covered benefits. This will depend on how many referral, specialty, or hospital services, laboratory,
imaging, and prescription drugs a patient needs in a given year beyond what the DPC offers. A
consumer with a HDHP must pay the full retail pricing, or discounted rates negotiated by their insurer,
for these additional services and medications until they meet the full amount of their deductible.
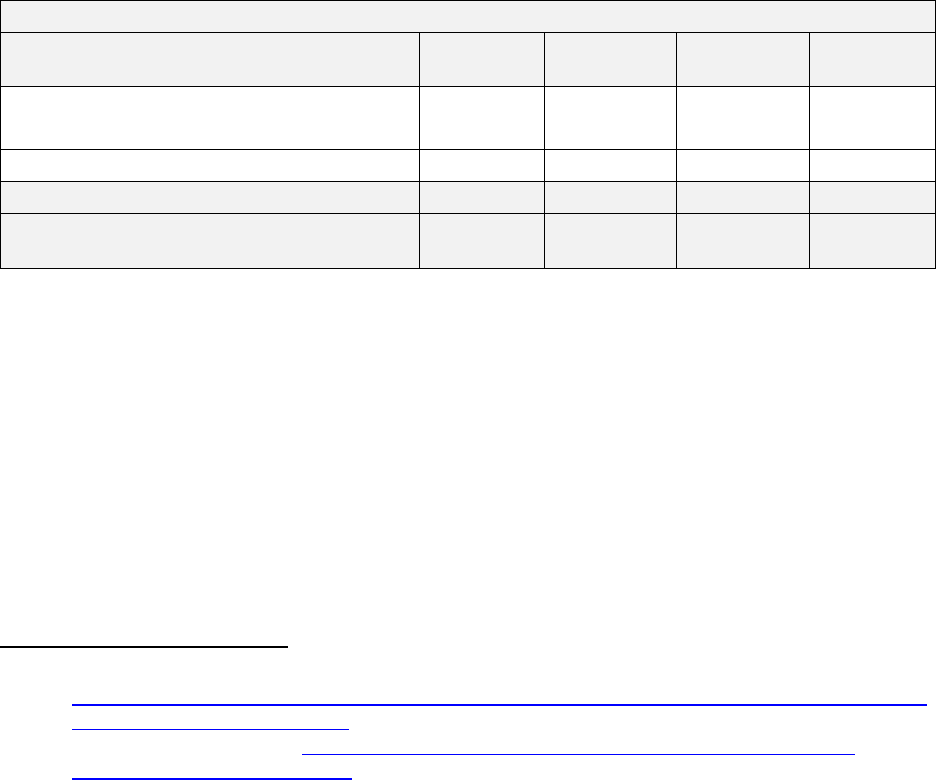
Table 3 displays the premiums for 2018 ACA-compliant coverage at the various ACA metal levels in
Wisconsin, before and after federal premium subsidies.
38
Most consumers (over 80%) purchasing
individual coverage qualify for premium subsidies, while 43% also qualified for cost-sharing reductions.
Table 3. Wisconsin 2018: Premiums, Before and After Federal Premium Subsidy, by Metal Level
Wisconsin 2018:
ACA-compliant e health plans on Exchange
Overall
Bronze Plan
Silver Plan
Gold Plan
Percent of Consumers Selecting Plans
(225,435 total consumers)
100%
33.4%
54.1%
11.4%
Average Premium (monthly)
$750
$626
$833
$759
Average premium after Subsidy (monthly)
$190
$209
$158
$278
Average Premiums after APTC among
consumers receiving APTC (monthly)
$106
$74
$105
$193
The deductive and scope of coverage HSA model and standard insurance model are comparable.
39
However, standard insurance plans generally offer coverage, prior to the consumer meeting deductible,
for a range of common services. For example, a Wisconsin standard commercial plan with a $5,000
deductible may cover primary and specialist office visits before deductible with a $25 copayment. The
HSA model generally requires the consumer to meet the full deductible before covering any services,
other than the ACA mandated preventive health services.
Table 4 displays the deductibles and copayments for sample HSA plays offered by Wisconsin issuers. The
HSA model offers potential savings due to its likely lower up-front premiums (although these premiums
may not be substantially lower if the consumer receives federal premium subsidies). The savings in
38
CMS, US DHHS. 2017 and 2018 Marketplace Open Enrollment Period Public Use Files.
https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Marketplace-
Products/Plan_Selection_ZIP.html
39
See national averages, reported at https://www.healthpocket.com/healthcare-research/infostat/2018-
obamacare-premiums-deductibles
UW Health Policy Group 13 | 20
premium payments for the HSA/HDHP-participant, in order to deliver value, will need to exceed the out-
of-pocket costs the consumer incurs that a standard might have covered.
Table 4. Sample 2018 HSA Individual and Family Plan Options, Wisconsin
40
Bronze HSA
Silver HSA
Gold HSA
Deductible – In Network (Single/Family) $6,650/$13,300 $3,200/$6,400 $1,800/$3,600
Out-of-Pocket– In Network
(Single/Family)
$6,650/$13,300 $6,550/$13,100 $6,550/$13,100
Coinsurance In-Network 0% 25% 10%
In-Network Preventive Care $0 $0 $0
In-Network Primary Care, Specialist,
Urgent Care, Emergency Room, and
Prescription Drugs
Deductible
Deductible with
Coinsurance
Deductible with
Coinsurance
Medicaid Coverage: Standard Medicaid vs. DPC plus Medicaid-wraparound
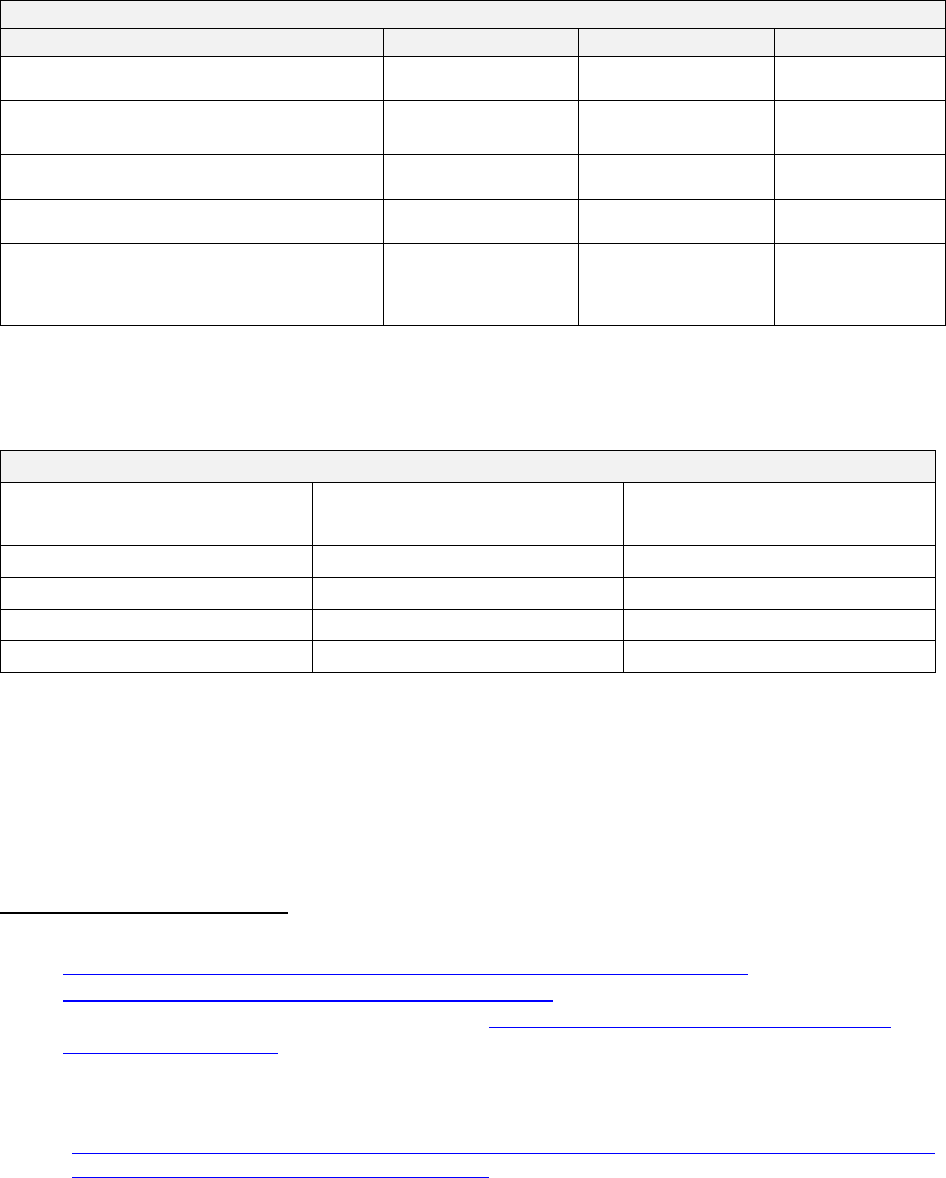
Table 5 displays the average benefit cost by eligibility group in Medicaid, for 2015-16.
41
Table 5. Average annual Wisconsin Medicaid per member per month cost, 2015-16
Average Annual Per Member
Cost
Average Per Member Per
Month (calculated by author)
Children
$1,762
$147
Parents
$4,128
$344
Childless Adults
$5,770
$481
BadgerCare Plus Total
$3,228
$269
The costs and benefits to the state budget would depend on the up-front costs of paying for the DPC
contracts, the extent to which primary care may be “carved out” of current managed care contracts, and
any reductions or increases in other medical or pharmacy service costs for individuals enrolled in
Medicaid DPC. As an example, if DHS implemented a DPC benefit that cost $70 per month (as
40
Samples from Quartz Health Plans:
https://unityhealth.com/docs/default-source/docs/uh01445-(0817)-primeoverview-
v5_final56382ad2b2e76b509b7eff0000a05e52.pdf?sfvrsn=2
and from Common Ground Healthcare Cooperative: https://www.commongroundhealthcare.org/our-
plans/individuals-families/
41
Wisconsin Legislative Fiscal Bureau. Medical Assistance and Related Programs (BadgerCare Plus, EBD Medicaid,
Family Care,and SeniorCare) Information Paper 41. Table 1.5: 2015-16 Total and Average Benefit Cost by
Eligibility Group. January 2017.
http://docs.legis.wisconsin.gov/misc/lfb/informational_papers/january_2017/0041_medical_assistance_a
nd_related_programs_informational_paper_41.pdf

UW Health Policy Group 14 | 20
contemplated in the original Wisconsin bill), the DPC model would need to reduce other Medicaid
benefit costs by at least $70 per month in order to save costs. This would depend on several factors:
• Do the health plans continue to price in the required preventive services into their
premiums, apart from the DPC, or carve out these services and rely on the DPC to provide
them?
• Does DPC provide and participate in after-hours care, or do their enrolled patients rely on
other sources of care for after-hours services?
• How much does the DPC rely on laboratory, imaging, and specialist referrals?
• Does the DPC model avert other specialty, lab, imaging, referral, and hospital costs that
would otherwise accrue to the Medicaid program?
V. Health System Value: Utilization, Quality, and Outcomes
Section IV details how the DPC value proposition depends on how much a DPC can handle a consumer’s
total health care needs relative to how much a consumer would need to spend outside of the monthly
DPC subscription fee to have sufficient coverage. This section considers how DPC might affect the
demand for and use of health care services, the quality of services delivered, and how this might relate
to health care and cost outcomes.
A. Volume of Care and Utilization
Most health care costs are concentrated in a small proportion of high-cost, high need patients – often
referred to as super-utilizers.
42
In fact, and the costliest five percent of patients account for half of all
health care spending. The superutilizer populations generally have complex chronic and acute needs. It
is not clear whether this population, their health care needs, and their costs can be managed within a
primary care office setting, as many of their needs require significant and intensive specialist
management and care coordination.
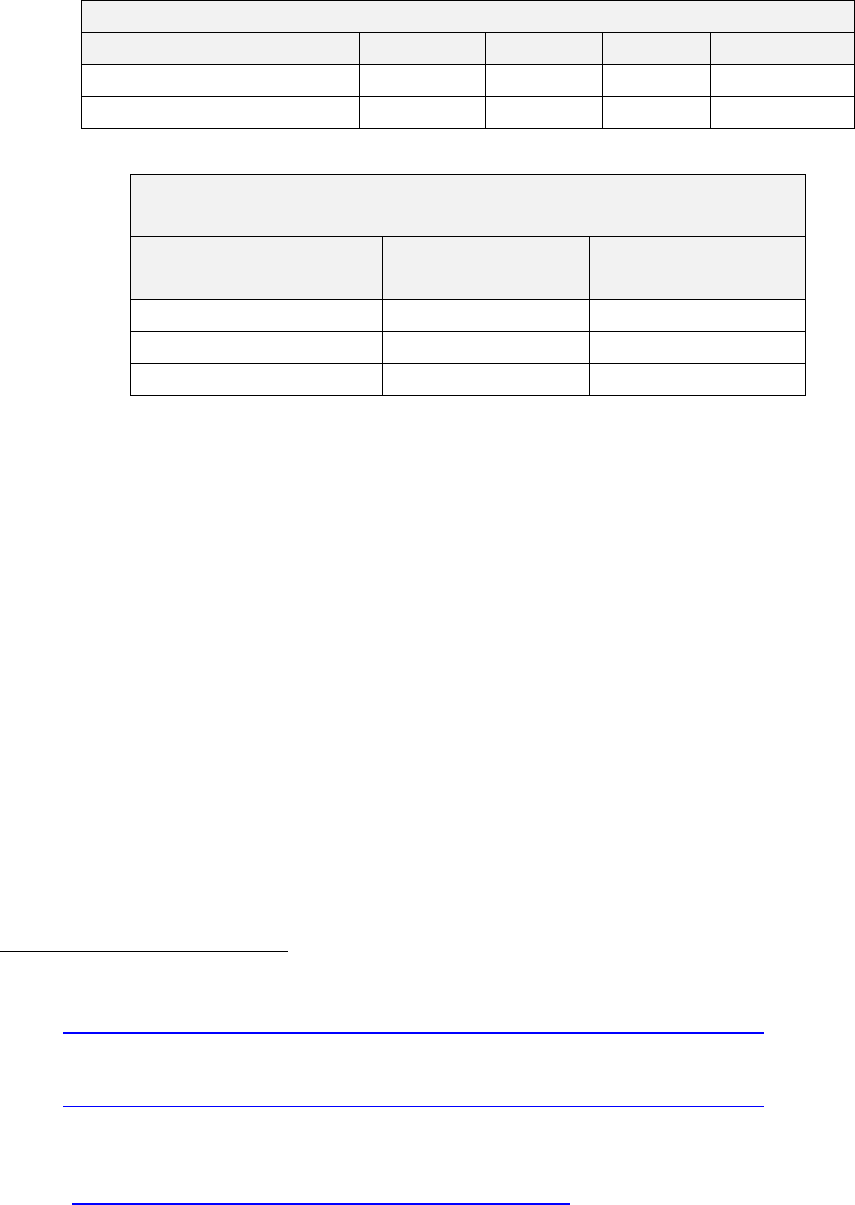
Most consumers, however, use relatively few health care services. About half of all U.S. residents visit
the physician three or fewer times in a year, while another quarter incur 4-9 visits annually.
43
(Table 6)
These include all visits – for primary and specialty care services. On a national level, 51% of those visits
occur with primary care physicians, 28% with another medical specialist and 21% with a surgical
42
Altarum Healthcare Value Hub. Addressing the Unmet Medical and Social Needs of Complex Patients.Reserach
Brief No. 17. February 2017.
http://www.healthcarevaluehub.org/advocate-
resources/publications/addressing-unmet-medical-and-social-needs-complex-patients/
43
U.S. CDC. Health, United States 2016. Table 65 Health care visits to doctor offices, emergency departments, and
home visits within the past 12 months, by selected characteristics: United States, selected years 1997–
2015. https://www.cdc.gov/nchs/data/hus/hus16.pdf#065
UW Health Policy Group 15 | 20
specialist;
44
on average in 2015, U.S. residents incurred 1.6 visits per year with primary care physicians,
and 1.5 visits per year to medical and surgical specialists.
45
(Table 7)
Table 6. Average Number of Physician Office Visits Annually
None
1-3
4-9
10 or more
Total Population
15.0%
48.4%
23.7%
12..8%
Medicaid
12.4%
43.4%
25.4%
18.8%
Table 7. Physician Office Visits 2015: Percent of Total Visits and
Average Number of Annual Visits Across Specialties
Specialty Type
Percent of Total
Visits
Average Number of
Visits
Primary Care
51.0%
1.60
Medical Specialty
28.4%
0.89
Surgical Specialty
20.6%
0.65
These figures suggest that most U.S. residents incur fewer than five primary care visits annually, and
about half would incur none, or only one or two visits, for which they would make use of their DPC
contract provider. The other half of their medical needs, along with the lab, imaging, and pharmacy
services associated with their primary care visits, may fall outside of the DPC contract and depend on
their insurance coverage and related cost-sharing exposure.
B. DPC Impact on Health Outcomes and Quality
Among recent trends in health care improvement and cost-containment, efforts have come to focus on
reducing overuse of services that lack a clear medical basis, which incur costs (and possible medical
harm) that exceed likely benefit.
46
It will be important to understand the degree to which DPC practices
provide evidence-based services to their members and avert costly services outside of the DPC that their
patients would otherwise have incurred.
DPC advocates assert that physicians are able to provide coordinated and comprehensive care, allow
access to physicians at any time, permit longer appointments with the physician, offer chronic disease
management, and provide cost-effective convenience.
47
As noted above, it remains unclear whether
44
National Ambulatory Medical Care Survey: 2015 State and National Summary Tables. Table 1. Physician office
visits, by selected physician characteristics.
https://www.cdc.gov/nchs/data/ahcd/namcs_summary/2015_namcs_web_tables.pdf
45
National Ambulatory Medical Care Survey: 2015 State and National Summary Tables. Table 1. Physician office
visits, by selected physician characteristics.
https://www.cdc.gov/nchs/data/ahcd/namcs_summary/2015_namcs_web_tables.pdf
46
Cassel CK, Guest JA. Choosing wisely: helping physicians and patients make smart decisions about their care.
JAMA. 2012;307(17):1801-1802.
47
Walton P. 5 benefits that concierge doctors offer. Clearwater, FL: American Academy of Private Physicians; 2014.
http://aapp.org/blog/5-benefits-that-concierge-doctors-offer
UW Health Policy Group 16 | 20
the extra time and additional visits available to the current DPC user population do in fact improve
health outcomes and avert other specialty and referral services that would otherwise occur. The
American College of Physicians, in its 2015 position paper,
48
warns as follows:
Retainer practices note that they are able to see their patients more often throughout the year. Once
again, there is no evidence to suggest that this is always necessary or effective. With all of the
“amenities” offered by these practices, it is important to do a cost–benefit analysis to understand the
true effect of the “extras” in a practice. At this time, no research or data are available to indicate
that many of these amenities in a practice yield better clinical outcomes. It is important to be aware
of the potential for overutilization of physician time and medical services.
DPCs not participating in insurance may not participate in quality measurement programs,
interoperability with other electronic health record systems, and the associated effect on quality and
outcomes.
49
It will be important for the DPC to report its encounter data to the health plan or other
monitoring entity, to allow ongoing quality review, and report its Medicaid and performance measures.
Lacking insurance regulation or payer oversight, DPC practices theoretically lack accountability to
professional review; “bad actors” could overload their practices with subscribing patients and
compromise on quality of care. Wisconsin’s DPC bill, as amended, would have relied on insurance plans
to regulate such conduct, specifying that direct primary care providers who wish to be part of an
insurance network must comply with the insurance carrier’s terms of participation.
VI. How do DPCs affect the primary care workforce?
U.S. primary care physicians maintain a practice panel of about 2,300 patients,
50
while DPCs typically
limit their patient panels to several hundred patients.
51,52,53
Direct primary care (DPC) allows physicians
to reduce their patient panel size and the daily volume of patients, while maintaining a competitive
income.
Proponents of DPC point to this decreased panel size, and increased time a provider can spend with
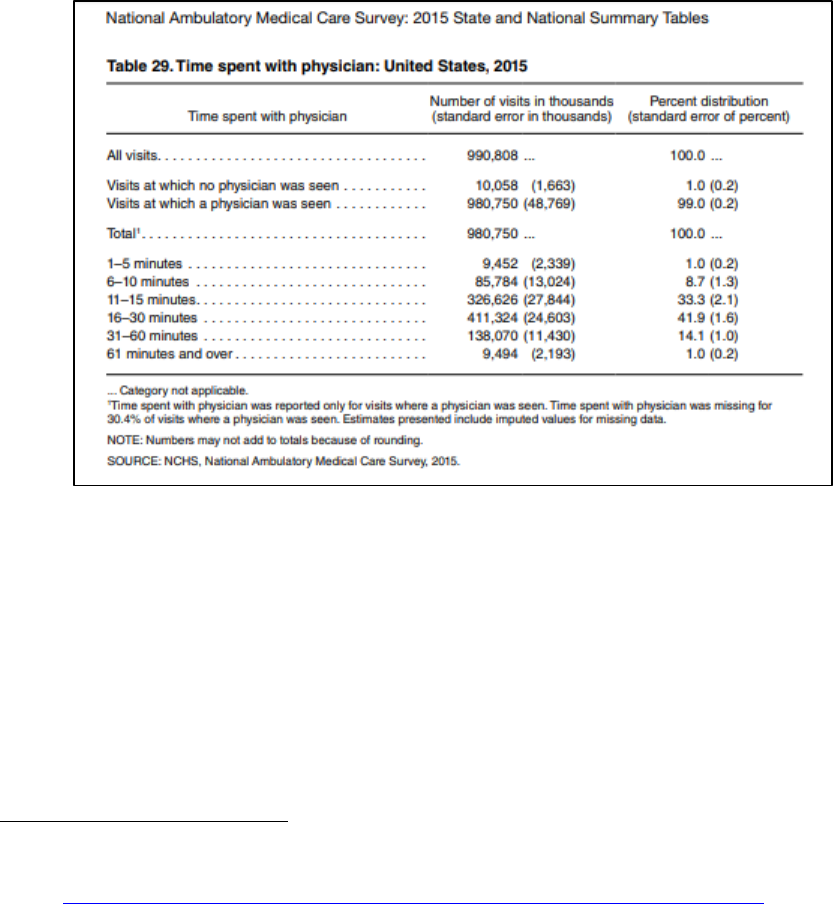
each patient, as one of the primary benefits of this model. Table 8 displays the time spent with
physicians in U.S. office visits, as reported in 2015.
54
About half last fewer than 15 minutes, 42% last up
48
Doherty R. Assessing the patient care implications of “concierge” and other direct patient contracting practices:
a policy position paper from the American College of Physicians. Ann Intern Med. 2015;163(2):949–952.
49
Ibid.
50
Altschuler J, Margolius D, Bodenheimer T, Grumbach K. Estimating a reasonable patient panel size for primary
care physicians with team-based task delegation. Ann Fam Med. 2012;10(5):396–400.
51
Qamar S. Direct primary care and concierge medicine: they're not the same KevinMD.com [blog]. 24 August
2014. www.kevinmd.com/blog/2014/08/direct-primary-care-concierge-medicine-theyre.html
52
Alexander GC, Kurlander J, Wynia MK. Physicians in retainer (“concierge”) practice. A national survey of
physician, patient, and practice characteristics. J Gen Intern Med. 2005;20(12):1079-1083.
53
Eskew P. In defense of Direct Primary Care. Am Pract Manag. 2016 Sep-Oct;23(5):12-14.
https://www.aafp.org/fpm/2016/0900/p12.html
54
NCHS, National Ambulatory Medical Care Survey, 2015. Table 29, Time spent with physicians: United States,
2015. https://www.cdc.gov/nchs/data/ahcd/namcs_summary/2015_namcs_web_tables.pdf
UW Health Policy Group 17 | 20
to 30 minutes, and about 15% last up to an hour. This will vary by specialty, with primary care specialties
averaging about 20 minutes overall.
55
In comparison, survey reports show that DPC physicians spend an average of 35 minutes with each
patient visit, and patients in the practice average four visits annually.
56
However, this comparison of
averages does not necessarily reflect an actual upgrade in service for each patient. The overall U.S.
average includes all patients, including those with high acuity and intensive service needs, averaged with
those that have few health care needs. Recall, as detailed above, that most of the population requires
very few health care visits annually while a minor proportion require a large number of visits.
Table 8.
Those persons with higher health care services needs very likely receive longer and more visits, while
those with fewer needs receive fewer and shorter visits. As well, primary care providers may refer those
with higher health care needs out to specialists for their additional health care visits. Some of those
referral services may be unnecessary and could be appropriately handled in the primary care setting,
while some may quite necessary given the needs of the patient.
In contrast, the DPC visit average includes only the limited population of patients enrolled in the DPC
subscription model. The DPC model, at this point, may in fact be enrolling an overall healthier patient
population; existing studies show enrolment of smaller proportions of African American and Hispanic
55
NCHS, National Ambulatory Medical Care Survey, 2015 Table 30. Time spent with physician, by physician
specialty: United States, 2015.
https://www.cdc.gov/nchs/data/ahcd/namcs_summary/2015_namcs_web_tables.pdf
56
Eskew P, Klink K. Direct primary care: practice distribution and cost across the nation. J Am Board Fam Med.
2015;28(6):793–801.

UW Health Policy Group 18 | 20
residents, and a tendency to locate in wealthier communities.
57
DPC patients may include the “worried
well” who appreciate DPC practice amenities and a relationship with the physician. But evidence does
not yet exist to show that, for these patients, more time with the physician or more visits improve
outcomes, or whether this population in fact needs these visits.
The extra time and visits provided by the DPC may not, for a generally well population, avert other
specialty or referral costs that would otherwise been incurred. If not, the DPC model would not
necessarily produce health care savings or reduce overall demand for services.
58
The DPC model lowers the patient-to-provider ratio, meaning a community needs more providers to
accommodate its population base at the primary care level. DPCs would need to reduce overall service
demand in the community to avoid creating or exacerbating workforce capacity shortages. If the extra
time and visits that DPCs provide for their patients do in fact alleviate need and demand for specialty
services, then the model could have a beneficial effect on the health care workforce.
DPC advocates also argue that the model can improve physician satisfaction and retention in practice.
They point to studies showing that U.S. physicians are among the least satisfied in the world.
59
Primary
care physicians express frustration with the limited the time they can spend with each patient and with
income stability,
60
along with the amount of time their practices spend on administrative burdens
related to insurance or payment claims.
61
DPC may encourage more physicians to stay in practice or
pursue primary care specialties.
62
Whether such potential primary care physician retention, or potential
increase in the supply, can sufficiently offset the reduction in patient-to-provider ratio within their
practices, remains uncertain.
57
Weisbart ES. Is Direct Primary Care the Solution to Our Health Care Crisis? Fam Pract Manag. 2016 Sep-
Oct;23(5):10-11. https://www.aafp.org/fpm/2016/0900/p10.html
58
Doherty R. Assessing the patient care implications of “concierge” and other direct patient contracting practices:
a policy position paper from the American College of Physicians. Ann Intern Med. 2015;163(2):949–952.
59
Commonwealth Fund International Health Policy Survey of Primary Care Physicians. New York, NY: The
Commonwealth Fund; November 2012.
http://www.commonwealthfund.org/interactives-and-data/chart-
cart/in-the-literature/2012-a-survey-of-primary-care-doctors-in-ten-countries/physician-satisfaction-with-
practicing-medicine
60
Friedberg MW, Chen PG, Van Busum KR, Aunon F, Pham C, Caloyeras J, et al. Factors affecting physician
professional satisfaction and their implications for patient care, health systems, and health policy. RAND.
2013. www.rand.org/pubs/research_reports/RR439.html
61
Osborn R, Moulds D, Schneider EC, et al. Primary Care Physicians In Ten Countries Report Challenges Caring For
Patients With Complex Health Needs. Health Affairs 2015; 34(12): 2104-2112.
62
Doherty R. Assessing the patient care implications of “concierge” and other direct patient contracting practices:
a policy position paper from the American College of Physicians. Ann Intern Med. 2015;163(2):949–952.

UW Health Policy Group 19 | 20
VII. Conclusion: Questions for Consideration
Many states, including Wisconsin, have adopted or are considering legislation to define DPC
arrangements as medical services rather than an insurance plan, and provide a framework for Medicaid
coverage of DPC services. The evidence has not yet established the effect of DPC on health care
spending, quality, or access.
As these discussions continue in Wisconsin, particularly regarding direction of Medicaid funding,
lawmakers may want to consider some of the following questions regarding the private insurance
market to guide their decisions:
Will DPC duplicate benefits provided through other private insurance coverage – particularly the
required preventive services that all insurance products must offer.
Will insurance premiums and products carve-out the preventive care component included in the
DPC subscription? If so, what is the effect on care coordination?
What are the actuarial projections for use of DPC services within the subscription fee relative to
the cost of other laboratory, imaging, prescription, drug, specialist referral, and hospital services
for which the consumer will experience cost exposure?
Does DPC avert additional care needs, such as hospitalization or prescription drug costs, such that
the consumer does not incur out-of-pocket costs that would have been covered under a standard
insurance plan?
Does this model reduce utilization and, thereby, costs in the health care system as a whole?
Can the DPC model sufficiently manage the care of high needs patients that currently incur most
of the costs within health care generally and specifically within the Medicaid program? Or
Are DPCs better positioned as an option for generally healthy, lower needs populations and, if so,
where do DPC’s find cost savings?
Given existing and projected primary care provider shortages, what effect would DPC expansion
have on access to care?
A Medicaid-DCP pilot program may additionally focus on the following questions:
• Would DPC affect the types of services needed by Medicaid enrollees, and would that the DPC
model generate savings to compensate for the cost of the DPC contracts?
• How would DPC affect current managed care contracts, and would carving out primary care
from those contracts affect care coordination and/or quality measurement?
UW Health Policy Group 20 | 20
VIII. Other Background Reading
1. American Academy of Family Practice: Director Primary Care.
https://www.aafp.org/practice-
management/payment/dpc.html
2. Baror R. Is Direct Primary Care the Future? Federal Bar Association.
http://www.fedbar.org/Sections/Health-Law-Section/Health-Law-Checkup/Is-Direct-Primary-Care-
the-Future.aspx
3. Engelhard CL Is direct primary care part of the solution or part of the problem? The Hill. October 13,
2014.
http://thehill.com/blogs/pundits-blog/healthcare/220527-is-direct-primary-care-part-of-the-
solution-or-part-of-the#bottom-story-socials
4. Friedberg MW et al. Effects of Health Care Payment Models on Physician l Practice in the United
States. RAND Corporation, 2015. https://www.rand.org/pubs/research_reports/RR869.html
5. Huff C. 2015. Affordability, Access, Models Of Care & More Direct Primary Care: Concierge Care For
The Masses. Health Affairs Vol. 34 (12): 2016-2019.
6. Kirchheimer S. The Doctor Will See You but Not Your Insurance. AARP. August 6, 2013.
https://www.aarp.org/health/health-insurance/info-08-2013/direct-primary-care.html
7. Levy R. Back to the Future: Implications of Recent Developments in Physician Payment
Methodologies. Journal of Health Care Compliance, September – October 2012, pp 55-71.
http://www.dickinson-wright.com/-/media/files/news/2012/09/back-to-the-future-implications-of-
recent-develo__/files/jhcc_05-12_levy/fileattachment/jhcc_05-12_levy.pdf?la=en
8. Luthra S. Would Paying Your Doctor Cash Up Front Get You Better Care? NPR, January 13, 2016.
https://www.npr.org/sections/health-shots/2016/01/13/462898517/can-concierge-medical-care-
work-for-the-middle-class
9. Ramsey L. A new kind of doctor's office that doesn't take insurance and charges a monthly fee is
'popping up everywhere' — and that could change how we think about healthcare. Business Insider.
March 17, 2018.
http://www.businessinsider.com/direct-primary-care-no-insurance-healthcare-
2018-3
10. Rosenbaum S. Law and the Public’s Health. Public Health Reports, Jan-Feb 2011, Vol 126: 130-135.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3001813/
11. Rubin R. Is Direct Primary Care a Game Changer? JAMA. 2018;319(20):2064-2066.
